When most people were thinking about summer vacation, we were contemplating the biggest science stories of 2018.
Yep, it takes more than six months of effort to put together Science News’ annual issue on the Top 10 science stories of the year. 2018 was no different, though we were hit with some exciting twists that had us revisiting our decisions just a week or so before closing the issue.
The early discussions tend to be more about themes — climate emerged as a big one, even before the recent reports linking increased severity of hurricanes, floods and wildfires to climate change. Reporters lobby to get the stories that intrigued them the most or the discoveries that mark critical turning points onto the short list. By August, our editors have identified contenders for the top of the list and are assigning stories so writers can get to work. We try to keep the choices under wraps; it’s part of the fun. All of the stories are assigned by October 1. By then, we’re also planning illustrations, graphics and bonus items, like our much-loved list of favorite science books of the year. By Thanksgiving, we’ve nailed down the “map” for the magazine, including story order and page designs.
And then news happens. This year was particularly rich in breaking news that had us reshuffling the deck. That included the discovery of an impact crater hidden under Greenland’s ice, which some scientists argue contributed to the die-off of the mammoths. That story broke on November 14 (SN: 12/8/18, p. 6).
Then there was the U.S. report on domestic climate change impacts, which was released the Friday after Thanksgiving. A few days later came an even bigger surprise: A Chinese scientist claimed that he had created the world’s first gene-edited babies. The announcement unleashed a torrent of criticism from scientists around the world. So what would you pick as the No. 1 science story of the year? After much discussion, our editorial team decided to stick with our original choice of climate change, considering the extraordinary amount of new data released this year and the import of those findings. The Chinese babies elbowed their way into the No. 2 slot. Even though the scientist’s claim may prove false, the technology has clearly advanced to the point where scientists and governments must act to set ethical standards for human gene editing.
Note to our readers: The magazine will be taking a break over the holidays. The next issue you receive will be dated January 19. But we’ll still be hard at work reporting on developments in science, medicine and technology; visit us at www.sciencenews.org for the latest. In 2019, we’ll publish four double issues, in May, July, October and December. These special issues include more features and in-depth coverage of topics like last summer’s “Water woes,” which included reporting from Mumbai, India. We love having the opportunity to dig deep on pressing issues and hope you enjoy the results. Thank you for being part of the Science News community. We wish you joyous holidays and an evidence-based new year.
In 2018, we saw just how much power science has to make a real impact.
Science News’ top stories of the year include a literal impact — the hidden contours of what appears to be a massive crater created when a meteorite slammed into Greenland long ago. That discovery ranks among our Top 10 partly because it’s just cool, but also because it raises the tantalizing prospect of solving a scientific mystery: Did the impact kick the planet into a roughly 1,000-year cold snap, called the Younger Dryas, almost 13,000 years ago? The mammoths and other species that died out by the end of that period didn’t see climate change coming. But we can. That’s why human-driven climate change is our top story of the year. The rising tide of attribution studies shows that climbing temperatures are already turning extreme events, such as Hurricane Florence, more extreme. This year’s barrage of climate reports gave us a clearer picture of how climate change will affect Earth in the near future — fueling wildfires, sparking heat waves, raising sea levels —and how human actions to curb warming can have an impact.
2018 is also the year a Chinese researcher made the startling claim that he had created the first babies to be born with an edited gene. The ensuing uproar over the controversial birth of twin girls in China, whose genes were allegedly tweaked to reduce their risk of contracting HIV, is sure to have a lasting impact on the future of gene-editing technology.
Two other genetics stories made our Top 10. Genetic genealogy is shaking up the field of forensics, ID’ing suspects in cold cases while raising privacy issues. And in a lab experiment, a gene drive — a genetic tool designed to be inherited by 100 percent of offspring — wiped out a population of mosquitoes. That feat ushers in the enticing but perilous possibility of both eliminating certain diseases and deliberately driving a species to extinction.
Other stories rounding out our Top 10 examine issues close to home (how to sort through conflicting advice about drinking alcohol) and very far away (tracing a high-energy neutrino back to its source in a distant galaxy). We’ll be watching these stories to see what happens in 2019 and beyond. — Macon Morehouse, News Director hurricane flooding SN TOP 10 1 Can half a degree save us? This is the year we learned that the 2015 Paris Agreement on global warming won’t be enough to forestall significant impacts of climate change. And a new field of research explicitly attributed some extreme weather events to human-caused climate change. This one-two punch made it clear that climate change isn’t just something to worry about in the coming decades. It’s already here. FULL STORY Jiankui He SN TOP 10 2 Gene-edited babies A Chinese scientist surprised the world in late November by claiming he had created the first gene-edited babies. Many researchers and ethicists say implanting gene-edited embryos to create babies is premature and exposes the children to unnecessary health risks. Critics also fear the creation of “designer babies.” FULL STORY Sacramento sheriff and Golden State killer SN TOP 10 3 Genealogy solves crimes In 2018, criminal investigators in the United States embraced genetic genealogy, a forensic technique for tracking down suspects through their family trees, to solve decades-old cold cases and some fresh crimes. But this new type of DNA-based detective work has raised questions about genetic privacy and police procedures. FULL STORY IceCube detector SN TOP 10 4 A neutrino’s distant source Mysterious particles called neutrinos constantly barrel down on Earth from space. No one has known where, exactly, the highest-energy neutrinos come from. This year, scientists finally put a finger on one likely source: a brilliant cosmic beacon called a blazar. The discovery could kick-start a new field of astronomy that combines information gleaned from neutrinos and light. FULL STORY Greenland crater illustration SN TOP 10 5 Impact crater unearthed For three years, a team of scientists kept a big secret: They had discovered a giant crater-shaped depression buried beneath about a kilometer of ice in northwestern Greenland. In November, the researchers revealed their find to the world. The crater may have reignited a debate over a controversial hypothesis about a mysterious cold snap known as the Younger Dryas. FULL STORY Anopheles gambiae mosquitoes SN TOP 10 6 The end of mosquitoes? For the first time, humans have built a set of pushy, destructive genes that infiltrated small populations of mosquitoes and drove them to extinction. This test and other news from 2018 feed one of humankind’s most persistent dreams: wiping mosquitoes off the face of the Earth. FULL STORY person covering wine glass SN TOP 10 7 Health risks of alcohol For people who enjoy an occasional cocktail, 2018 was a sobering year. Headlines delivered the news with stone-cold certainty: Alcohol — in any amount — is bad for your health. “The safest level of drinking is none,” a group of scientists concluded. FULL STORY Mars south pole SN TOP 10 8 Mars’ ice-covered lake Researchers reported this year that they found a wide lake of standing liquid near the Red Planet’s south pole, buried beneath 1.5 kilometers of ice. The purported polar pool is the largest volume of liquid water ever claimed to currently exist on Mars, and has probably been around for a long time. Both of those features raise hopes that life could survive on Mars today. FULL STORY Gert-Jan Oskam walking with crutches SN TOP 10 9 Progress against paralysis Intensive rehabilitation paired with electric stimulation of the spinal cord allowed six paralyzed people to walk or take steps years after their injuries, three small studies published this year showed. More importantly, they show that the spinal cord can make a comeback. FULL STORY painting on cave walls in Spain SN TOP 10 10 Origins of human smarts Archaeological discoveries reported this year broadened the scope of what scientists know about Stone Age ingenuity. These finds move the roots of innovative behavior ever closer to the origins of the human genus. FULL STORY
Behavioral ecologist Anna Holzner recalls first seeing a southern pig-tail macaque munching on a headless rat. These monkeys were known to eat fruits, insects and even dirt, but nobody had reported them eating rats. “It was funny,” says Holzner, “and disgusting.”
This unexpected act occurred dozens of times from March to August 2016 as Holzner, of the University of Leipzig in Germany, and colleagues recorded what the macaques ate on oil palm plantations in northwest Peninsular Malaysia. To planters there, the macaques are pests.
Holzner did the work as part of the Macaca Nemestrina Project led by primate ecologist Nadine Ruppert of Universiti Sains Malaysia, in Penang. She presented the results on July 2 at the annual meeting of the Association of Tropical Biology and Conservation in Kuching, Malaysia.
While pig-tail macaques, Macaca nemestrina, spend most of their time in the forest, they visit adjacent plantations daily to forage, report Ruppert, Holzner and others in a related study in the April 4 International Journal of Primatology.
Holzner’s new study shows that in the plantations, pig-tail macaques ate mostly oil palm fruits, spending only 1 percent of their meal times on rats. But the monkeys would peel open the bark on oil palm trunks to expose rats hiding within. The researchers estimate that a group of 30 macaques might eat as many as 2,080 rats in a year. Holzner’s team counted fewer rats wherever they located macaques.
The study has local plantation owners reconsidering the monkeys, which may not be pests after all, but agents of rat control, Holzner says. But as macaques adapt to the encroaching plantations and their numbers grow, they can reduce birds and other creatures living in adjacent forests, warns ecologist Matthew Luskin at the Nanyang Technological University in Singapore.
Today’s young women are more likely to experience depression and anxiety during pregnancy than their mothers were, a generation-spanning survey finds.
From 1990 to 1992, about 17 percent of young pregnant women in southwest England who participated in the study had signs of depressed mood. But the generation that followed, including these women’s daughters and sons’ partners, fared worse. Twenty-five percent of these young women, pregnant in 2012 to 2016, showed signs of depression, researchers report July 13 in JAMA Network Open. “We are talking about a lot of women,” says study coauthor Rebecca Pearson, a psychiatric epidemiologist at Bristol University in England.
Earlier studies also had suggested that depression during and after pregnancy is relatively common (SN: 3/17/18, p. 16). But those studies are dated, Pearson says. “We know very little about the levels of depression and anxiety in new mums today,” she says.
To measure symptoms of depression and anxiety, researchers used the Edinburgh Postnatal Depression Scale — 10 questions, each with a score of 0 to 3, written to reveal risk of depression during and after pregnancy. A combined score of 13 and above signals high levels of symptoms.
From 1990 to 1992, 2,390 women between the ages of 19 and 24 took the survey while pregnant. Of these women, 408 — or 17 percent — scored 13 or higher, indicating worrisome levels of depression or anxiety. When researchers surveyed the second-generation women, including both daughters of the original participants and sons’ partners ages 19 to 24, the numbers were higher. Of 180 women pregnant in 2012 to 2016, 45 of them — or 25 percent — scored 13 or more. It’s not clear whether the findings would be similar for pregnant women who are older than 24 or younger than 19. That generational increase in young women scoring high for symptoms of depression comes in large part from higher scores on questions that indicate anxiety and stress, Pearson says. Today’s pregnant women reported frequent feelings of “unnecessary panic or fear” and “things getting too much,” for instance.
Those findings fit with observations by psychiatrist Anna Glezer of the University of California, San Francisco. “A very significant portion of my patients present with their primary problem as anxiety, as opposed to a low mood,” says Glezer, who has a practice in Burlingame, Calif.
The study’s cutoff score for indicating high depression risk was 13, but Pearson points out that a lower score can signal mild depression. Women who score an 8 or 9 “still aren’t feeling great,” she says. It’s likely that even more pregnant women might have less severe, but still unpleasant symptoms, she says.
The researchers also found that depression moves through families. Daughters of women who were depressed during pregnancy were about three times as likely to be depressed during their own pregnancy than women whose mothers weren’t depressed. That elevated risk “was news to me,” says obstetrician and gynecologist John Keats, who chaired a group of the American College of Obstetricians and Gynecologists that studied maternal mental health. Asking about whether a patient’s mother experienced depression or anxiety while pregnant might help identify women at risk, he says.
Negative effects of stress can be transmitted during pregnancy in ways that scientists are just beginning to understand, and stopping this cycle is important (SN Online: 7/9/18). “You’re not only talking about the effects on a patient and her family, but potential effects on her growing fetus and newborn,” says Keats, of the David Geffen School of Medicine at UCLA.
Although researchers don’t yet know what’s behind the increase, they have some guesses. More mothers work today than in the 1990s, and tougher financial straits push women to work inflexible jobs. More stress, less sleep and more time sitting may contribute to the difference.
Time on social media may also increase feelings of isolation and anxiety, Glezer says. Social media can help new moms get information, but that often comes with “a whole lot of comparisons, judgments and expectations.”
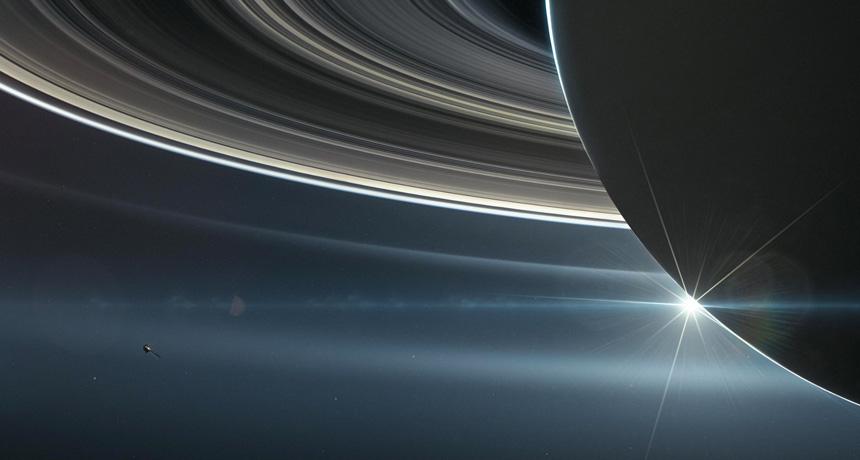
Data from NASA’s now-defunct Cassini spacecraft show that five odd-shaped moons embedded in Saturn’s rings are different colors, and that the hues come from the rings themselves, researchers report. That observation could help scientists figure out how the moons were born.
“The ring moons and the rings themselves are kind of one and the same,” says planetary scientist Bonnie Buratti of NASA’s Jet Propulsion Laboratory in Pasadena, Calif. “For as long as the moons have existed, they’ve been accreting particles from the rings.” Saturn has more than 60 moons, but those nearest to the planet interact closely with its main band of rings. Between December 2016 and April 2017, Cassini passed close to five of these ring-dwelling moons: ravioli-shaped Pan and Atlas (SN Online: 3/10/17), ring-sculpting Daphnis and Pandora (SN: 9/2/17, p. 16) and potato-shaped Epimetheus. The flybys brought Cassini between two and 10 times closer to the moons than it had ever been, before the spacecraft deliberately crashed into Saturn in September 2017 (SN Online: 9/15/17).
Examining those close-ups, Buratti and her colleagues noticed that the moons’ colors vary depending on the objects’ distances from Saturn. And the moon hues are similar to the colors of the rings that the objects are closest to, the team reports online March 28 in Science. Close-in Pan was the reddest moon, while the farthest-out Epimetheus was the bluest. The researchers think the red material comes from Saturn’s dense main rings, and mostly consists of organics and iron (SN Online: 10/4/18). The blue material is probably water ice from Saturn’s more distant E ring, which is created by plumes erupting from the larger, icy moon Enceladus. The team thinks that the rings are continually depositing material onto the moons. “It’s an ongoing process,” Buratti says. She notes that “skirts” of material at Atlas and Pan’s equators are probably made of accreted ring debris, too.
The overall similarity between the moons and rings led the researchers to conclude that these small moons are leftover shards of a destructive event that created the rings in the first place. But it’s unknown whether that event was a collision between long-gone, larger moons, the shredding of one moon by Saturn’s gravity, or some other occurrence (SN: 1/20/18, p. 7).
Saturn, its rings and its moons are “very dynamic,” says planetary scientist Matija Ćuk of the SETI Institute in Mountain View, Calif. The idea that the rings are still shedding material onto the moons today “sounds perfectly reasonable.” He isn’t sure the moons formed at the same time as the rings, though. It’s possible “they formed from the rings since that catastrophic event,” he says.
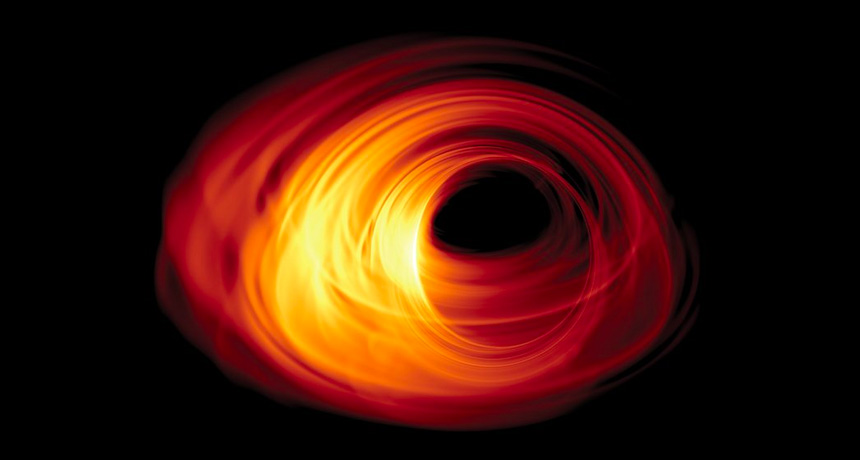
Editor’s note: On April 10, the Event Horizon Telescope collaboration released a picture of the supermassive black hole at the center of galaxy M87. Read the full story here.
We’re about to see the first close-up of a black hole.
The Event Horizon Telescope, a network of eight radio observatories spanning the globe, has set its sights on a pair of behemoths: Sagittarius A*, the supermassive black hole at the Milky Way’s center, and an even more massive black hole 53.5 million light-years away in galaxy M87 (SN Online: 4/5/17). In April 2017, the observatories teamed up to observe the black holes’ event horizons, the boundary beyond which gravity is so extreme that even light can’t escape (SN: 5/31/14, p. 16). After almost two years of rendering the data, scientists are gearing up to release the first images in April.
Here’s what scientists hope those images can tell us.
What does a black hole really look like? Black holes live up to their names: The great gravitational beasts emit no light in any part of the electromagnetic spectrum, so they themselves don’t look like much.
But astronomers know the objects are there because of a black hole’s entourage. As a black hole’s gravity pulls in gas and dust, matter settles into an orbiting disk, with atoms jostling one another at extreme speeds. All that activity heats the matter white-hot, so it emits X-rays and other high-energy radiation. The most voraciously feeding black holes in the universe have disks that outshine all the stars in their galaxies (SN Online: 3/16/18). The EHT’s image of the Milky Way’s Sagittarius A, also called SgrA, is expected to capture the black hole’s shadow on its accompanying disk of bright material. Computer simulations and the laws of gravitational physics give astronomers a pretty good idea of what to expect. Because of the intense gravity near a black hole, the disk’s light will be warped around the event horizon in a ring, so even the material behind the black hole will be visible. And the image will probably look asymmetrical: Gravity will bend light from the inner part of the disk toward Earth more strongly than the outer part, making one side appear brighter in a lopsided ring.
Does general relativity hold up close to a black hole? The exact shape of the ring may help break one of the most frustrating stalemates in theoretical physics.
The twin pillars of physics are Einstein’s theory of general relativity, which governs massive and gravitationally rich things like black holes, and quantum mechanics, which governs the weird world of subatomic particles. Each works precisely in its own domain. But they can’t work together.
“General relativity as it is and quantum mechanics as it is are incompatible with each other,” says physicist Lia Medeiros of the University of Arizona in Tucson. “Rock, hard place. Something has to give.” If general relativity buckles at a black hole’s boundary, it may point the way forward for theorists.
Since black holes are the most extreme gravitational environments in the universe, they’re the best environment to crash test theories of gravity. It’s like throwing theories at a wall and seeing whether — or how — they break. If general relativity does hold up, scientists expect that the black hole will have a particular shadow and thus ring shape; if Einstein’s theory of gravity breaks down, a different shadow.
Medeiros and her colleagues ran computer simulations of 12,000 different black hole shadows that could differ from Einstein’s predictions. “If it’s anything different, [alternative theories of gravity] just got a Christmas present,” says Medeiros, who presented the simulation results in January in Seattle at the American Astronomical Society meeting. Even slight deviations from general relativity could create different enough shadows for EHT to probe, allowing astronomers to quantify how different what they see is from what they expect. Do stellar corpses called pulsars surround the Milky Way’s black hole? Another way to test general relativity around black holes is to watch how stars careen around them. As light flees the extreme gravity in a black hole’s vicinity, its waves get stretched out, making the light appear redder. This process, called gravitational redshift, is predicted by general relativity and was observed near SgrA* last year (SN: 8/18/18, p. 12). So far, so good for Einstein.
An even better way to do the same test would be with a pulsar, a rapidly spinning stellar corpse that sweeps the sky with a beam of radiation in a regular cadence that makes it appear to pulse (SN: 3/17/18, p. 4). Gravitational redshift would mess up the pulsars’ metronomic pacing, potentially giving a far more precise test of general relativity.
“The dream for most people who are trying to do SgrA* science, in general, is to try to find a pulsar or pulsars orbiting” the black hole, says astronomer Scott Ransom of the National Radio Astronomy Observatory in Charlottesville, Va. “There are a lot of quite interesting and quite deep tests of [general relativity] that pulsars can provide, that EHT [alone] won’t.”
Despite careful searches, no pulsars have been found near enough to SgrA* yet, partly because gas and dust in the galactic center scatters their beams and makes them difficult to spot. But EHT is taking the best look yet at that center in radio wavelengths, so Ransom and colleagues hope it might be able to spot some.
“It’s a fishing expedition, and the chances of catching a whopper are really small,” Ransom says. “But if we do, it’s totally worth it.” How do some black holes make jets? Some black holes are ravenous gluttons, pulling in massive amounts of gas and dust, while others are picky eaters. No one knows why. SgrA* seems to be one of the fussy ones, with a surprisingly dim accretion disk despite its 4 million solar mass heft. EHT’s other target, the black hole in galaxy M87, is a voracious eater, weighing in at between about 3.5 billion and 7.22 billion solar masses. And it doesn’t just amass a bright accretion disk. It also launches a bright, fast jet of charged subatomic particles that stretches for about 5,000 light-years.
“It’s a little bit counterintuitive to think a black hole spills out something,” says astrophysicist Thomas Krichbaum of the Max Planck Institute for Radio Astronomy in Bonn, Germany. “Usually people think it only swallows something.”
Many other black holes produce jets that are longer and wider than entire galaxies and can extend billions of light-years from the black hole. “The natural question arises: What is so powerful to launch these jets to such large distances?” Krichbaum says. “Now with the EHT, we can for the first time trace what is happening.”
EHT’s measurements of M87’s black hole will help estimate the strength of its magnetic field, which astronomers think is related to the jet-launching mechanism. And measurements of the jet’s properties when it’s close to the black hole will help determine where the jet originates — in the innermost part of the accretion disk, farther out in the disk or from the black hole itself. Those observations might also reveal whether the jet is launched by something about the black hole itself or by the fast-flowing material in the accretion disk.
Since jets can carry material out of the galactic center and into the regions between galaxies, they can influence how galaxies grow and evolve, and even where stars and planets form (SN: 7/21/18, p. 16).
“It is important to understanding the evolution of galaxies, from the early formation of black holes to the formation of stars and later to the formation of life,” Krichbaum says. “This is a big, big story. We are just contributing with our studies of black hole jets a little bit to the bigger puzzle.”
Editor’s note: This story was updated April 1, 2019, to correct the mass of M87’s black hole; the entire galaxy’s mass is 2.4 trillion solar masses, but the black hole itself weighs in at several billion solar masses. In addition, the black hole simulation is an example of one that uphold’s Einstein’s theory of general relativity, not one that deviates from it.
As the morning sun peeked through the trees, Rodger Kram readied himself for the coming marathon. But not the kind he used to run.
Kram, a physiologist at the University of Colorado Boulder, stood next to undergrad James Wilson at the end of a rural dirt road. Each donned a strap of nylon webbing onto his head. Attached to the bottom of their straps — called tumplines — a log rested horizontally across the duo’s lower backs. The pair was about to embark on a 25-kilometer trek to replicate how the ancient people of Chaco Canyon may have transported timber around 1,000 years ago (SN: 5/17/17). By the end of the day, their successful journey suggested that it would have taken just a few days for three people with tumplines to carry a full-size timber to Chaco, Kram, Wilson and colleagues reported on February 22 in the Journal of Archaeological Science: Reports.
Located in the northwest corner of New Mexico, Chaco Canyon is home to grand structures built between A.D. 850 and 1200. Multistoried stone buildings called great houses had roofs with timber beams about 5 meters long and 22 centimeters in diameter. The site contained at least 200,000 timbers of this size. But the wood came from forests more than 75 kilometers away (SN: 9/26/01). Load-pulling animals and wheels weren’t there at the time, and the timbers don’t appear to have been dragged. Scientists are puzzled by how the ancient people, ancestors of modern-day Diné and Pueblo peoples, moved the large timbers.
A 1986 study suggested that each log used as a beam had a mass of 275 kilograms. But Kram suspected this number couldn’t be correct.
In 2016, he cut a section of a tree outside of his house — ponderosa pine, the same species used in Chaco — and weighed it on his bathroom scale. He then extrapolated that a 5-meter-long timber would be closer to 90 kilograms. This revelation led to a 2022 study recalculating the masses of the Chaco Canyon timbers as between 85 and 140 kilograms.
“As soon as we figured out that the weight was reasonable, I wanted to carry them,” Kram says.
He and Wilson proposed that tumplines could have been used to transport the timbers. These head straps have been found on every inhabited continent and are thought to have been used since at least around 2,000 years ago. They are still widely used to carry heavy loads, such as by professional porters in Nepal. A tumpline is placed on the crown of the head — to be in line with the cervical spine — with the attached cargo resting on the small of the back. While there is no evidence that the people of Chaco used tumplines to haul timbers, there is proof that they used them to transport other items, like water vessels.
To see if tumpline timber transportation was humanly possible, Kram and Wilson trained for three months during the summer of 2020, gradually increasing their load weight and walk duration. Strangers who passed by couldn’t hide their confusion.
On the final day, the pair walked 25 kilometers while carrying a ponderosa pine that had been air-dried, which is how the people of Chaco may have prepared timbers. The 60-kilogram log was 2.5 meters long and 24 centimeters in diameter. The entire trek took almost 10 hours, and the weight of the full timber only slightly slowed the duo’s pace.
“I felt happy at the end that it was proved feasible, and that the 132-pound log we shared was off our necks,” says Wilson, now a medical student at the University of Colorado School of Medicine in Aurora. But “I never really doubted that we could do it.”
In the classic fairy tale, Hansel and Gretel dropped bread crumbs while walking through a treacherous forest so they wouldn’t lose their way. Rovers may one day use a similar trick to traverse other planets without losing their data.
Typically, if a rover permanently loses communication during a mission, all the information that it has gathered is lost. To avoid this, researchers suggest using a multi-rover system in which a smaller rover piggybacks on a larger “mother rover.” The smaller rover would then venture into any especially uncertain territory, such as a cave or lava tubes, deploying sensors the size of an AirPods case like bread crumbs as it goes. The sensors could then communicate with each other via a wireless network and funnel any collected data back to the mother rover, theoretical physicist Wolfgang Fink and colleagues propose February 11 in Advances in Space Research. As proof of concept, the team built prototype sensors that communicate via Wi-Fi.
It’s not that the smaller rover would be following the “bread crumbs” back the way it came. Instead, “we use [the sensors] for the data to find its way communication-wise out of the cave to the mother rover,” says Fink, of the University of Arizona in Tucson.
The technology could also be useful here on Earth, especially after a natural disaster such as an earthquake. A rover could be sent with the deployable sensors into rubble where it’s too dangerous for people to perform search-and-rescue missions (SN: 12/3/14).
The bread crumb–like communication network could allow researchers to “cater to the essence of scientific exploration,” Fink says, by allowing rovers to overcome some of the constraints posed by tricky terrain. “To get to the real exciting science, you most of the time have to go to exotic places, hard-to-get-to places.”
An uncomfortable truth is that there is another influenza pandemic in humankind’s future. Whether it will be a relative of the lethal avian flu strain currently wreaking havoc in bird populations around the globe is anyone’s guess.
Because the virus, called H5N1, can be deadly to birds, mammals and people, researchers closely monitor reports of new cases. Worryingly, a new variant of H5N1 that emerged in 2020 has not only spread farther than ever before among birds, but has also spilled over into other animals, raising the specter of a human outbreak (SN: 12/12/22).
The variant was linked to a seal die-off in Maine last summer. In October, there was an H5N1 outbreak on a mink farm in Spain, researchers reported in January in Eurosurveillance. (It’s unclear how the mink were exposed, but the animals were fed poultry by-products.) Sea lions off the coast of Peru and wild bears, foxes and skunks, which prey upon or scavenge birds, in the United States and Europe have also tested positive for the virus.
Globally, hundreds of millions of domestic poultry have been culled or died from the new variant. It’s also likely that millions of wild birds have died, though few governmental agencies are counting, says Michelle Wille a viral ecologist at the University of Sydney who studies avian influenza. “This virus is catastrophic for bird populations.”
A handful of human cases have also been reported, though there’s no evidence that the virus is spreading among people. Of seven cases, six people recovered and one person from China died. In February, health officials in China reported an eighth case in a woman whose current condition is unknown.
What’s more, four of the reported human cases — including a U.S. case from Colorado and two workers linked to the Spanish mink farm — were in people who didn’t have any respiratory symptoms. That leaves open the possibility that those people were not truly infected. Instead, tests may have picked up viral contamination, say in the nose, that the people breathed in while handling infected birds.
The impossibility of predicting which avian influenza viruses might make the jump to people and spark an outbreak is in part related to knowledge gaps. These bird pathogens don’t typically easily infect or circulate among mammals including humans. And scientists don’t have a full grasp on how these viruses might need to change for human transmission to occur.
For now, it’s encouraging that so few people have gotten infected amid such a large outbreak among birds and other animals, says Marie Culhane, a food animal veterinarian at the University of Minnesota in St. Paul. Still, experts around the globe are diligently watching for any signs the virus may be evolving to spread more easily between people.
The good news is that flu drugs and vaccines that work against the virus already exist, Wille says. Compared with where the world was when the coronavirus behind the COVID-19 pandemic came on the scene, “we are already ahead of the game.”
How the virus would need to change to spread among people is a big unknown This new iteration of bird flu is what’s called a highly pathogenic avian influenza, one that is particularly lethal for both domestic and wild birds. Aquatic birds such as ducks naturally carry avian flus with no or minor signs of infection. But when influenza viruses shuffle between poultry and waterfowl, variants with changes that make them lethal to birds can emerge and spread.
Avian viruses can be severe or even deadly for people. Since 2003, there have been 873 human cases of H5N1 infections reported to the World Health Organization. A little less than half of those people died. In February, an 11-year-old girl in Cambodia died after she developed severe pneumonia from an avian flu virus, the country’s first reported infection since 2014. Her father was also infected with the virus — a different variant than the one behind the widespread outbreak in birds —though he has not developed symptoms. It’s unknown how the two people were exposed.
Some of what scientists know about H5N1’s pandemic potential comes from controversial research on ferrets done more than a decade ago (SN: 6/21/13). Experiments showed that some changes to proteins that help the virus break into cells and make more copies of itself could help the virus travel through the air to infect ferrets, a common laboratory stand-in for humans in influenza research.
While researchers know these mutations are important in lab settings, it’s still unclear how crucial those changes are in the real world, says Jonathan Runstadler, a disease ecologist and virologist at Tufts University’s Cummings School of Veterinary Medicine in North Grafton, Mass. Viruses change constantly, but not all genetic tweaks work together. A change may help one version of the virus transmit better, while also hurting another variant and making it less likely to spread.
“We’re not sure how critical or how big a difference or how much to worry about those mutations when they happen in the wild,” Runstadler says. “Or when they happen five years down the road when there are other changes in the virus’s genetic background that are impacting those [original] mutations.”
That doesn’t stop researchers from trying to pinpoint specific changes. Runstadler and his team look for viruses in nature that have jumped into new animals and work backward to figure out which mutations were crucial. And virologist Louise Moncla says her lab is trying to develop ways to scan entire genetic blueprints of viruses from past outbreaks to look for signatures of a virus that can jump between different animal species.
“There’s a ton that we don’t know about avian influenza viruses and host switching,” says Moncla, of the University of Pennsylvania.
Genetic analyses of H5N1 circulating on the mink farm in Spain, for instance, revealed a change known to help the virus infect mice and mammalian cells grown in the lab. Such a change could make it easier for the virus to spread among mammals, including people. There could have been mink-to-mink transmission on the farm, the researchers concluded, but it remains unclear how much of a role that specific mutation played in the outbreak.
It’s a numbers game for when influenza viruses with the ability to transmit among mammals might make the jump from birds, Runstadler says. “The more chances you give the virus to spill over and adapt, the higher the risk will be that one of those adaptations will be effective [at helping the virus spread among other animals] or take root and be a real problem.”
The ongoing outbreak is still a big problem for birds Irrespective of our inability to forecast human’s future with H5N1, it’s clear that many species of birds — and some other animals that eat them — are dying now. And more species of birds are dying in this outbreak than previous ones, Culhane and Wille say.
“We have seen huge outbreaks in raptors and seabirds, which were never really affected before,” Wille says. It’s possible that genetic changes have helped the virus to spread more efficiently among birds than previous versions of H5N1, but that’s unknown. “There are a number of studies underway to try and figure it out,” Wille says. Historically, these deadly avian flus have not been a persistent problem in the Americas, Moncla says. Sporadic outbreaks of H5N1 variants are typically limited to places such as parts of Asia, where the virus has circulated in birds since its emergence in the late 1990s, and northern Africa.
North America’s last big avian flu outbreak was in 2015, when experts detected more than 200 cases of a different bird flu virus in commercial and backyard poultry across the United States. The poultry industry culled more than 45 million birds to stop that virus’s spread, Culhane says. “But it didn’t go away from the rest of the world.”
The latest version of H5N1 arrived on North American shores from Europe in late 2021, first popping up in Canada in Newfoundland and Labrador. From there, it spread south into the United States, where so far tens of millions of domestic poultry have been culled to prevent transmission on farms where the virus has been detected. By December 2022, the virus had made it to South America. In Peru, tens of thousands of pelicans and more than 700 sea lions have died since mid-January.
It’s important to understand exactly how nonbird animals are getting exposed, Culhane says. Highly pathogenic avian influenzas infect every organ of a bird’s body. So, a fox chowing down on an infected bird is exposing its own mouth, nose and stomach to a lot of virus as it eats its meal.
For now, experts are keeping an eye on infected animals to raise the alarm early if H5N1 starts transmitting among mammals.
“I do think that the mink outbreak, and then the sea lion outbreak, is a wake-up call,” Moncla says. “We should be doing our very best to implement all the science we can to try and understand what’s happening with these viruses so that if the situation does change, we are better prepared.”
LAS VEGAS — It’s a bold claim: The quest to create a superconductor that works under practical conditions is finally fulfilled, a team of researchers says. But controversy has dogged the team’s earlier claim of record-breaking superconductivity, and the new result is already facing extreme scrutiny.
The ultimate test will be whether the result can be confirmed by other researchers, says physicist Mikhail Eremets of the Max Planck Institute for Chemistry in Mainz, Germany. “I repeat it like [a] mantra: ‘Reproduce.’” Many materials become superconductors, able to transmit electricity with no resistance, provided they’re cooled to very low temperatures. A few superconductors work under warmer conditions, but those must be squeezed to crushing pressures, so they’re impractical to use.
Now physicist Ranga Dias of the University of Rochester in New York and colleagues say they have created a superconductor that works at both room temperature and relatively low pressure. A superconductor that operates under such commonplace conditions could herald a new age of high-efficiency machines, supersensitive instrumentation and revolutionary electronics.
“This is the start of the new type of material that’s useful for practical applications,” Dias said March 7 at the American Physical Society meeting, where he reported the feat.
The superconductor is made of hydrogen mixed with nitrogen and a rare earth element called lutetium, Dias and colleagues report March 8 in Nature. The team combined the elements and squeezed them in a device known as a diamond anvil cell. The researchers then varied the pressure and temperature and measured the resistance to electrical flow in the compound.
At temperatures as high as 294 kelvins (about 21° Celsius or 70° Fahrenheit), the material seemed to lose any electrical resistance. It still required pressures of 10 kilobar, which is about 10,000 times the pressure of Earth’s atmosphere. But that’s far lower than the millions of atmospheres of pressure typically required for superconductors that operate near room temperature. If confirmed, that makes the material much more promising for real-world applications.
The material displayed several hallmarks of a superconductor, the team reports. Not only did the electrical resistance suddenly drop as it became superconducting, but the material also expelled magnetic fields and exhibited an abrupt change in its heat capacity, Dias says.
When the researchers put the squeeze on the material in the diamond anvil cell, it suddenly turned from a bluish hue to hot pink. “I had never seen a color change like this in a material,” Dias says. “It was like, wow.” That color change indicated a shift in the electrical properties of the material as it became a superconductor, Dias says. This superconductor might be able to escape the confines of a diamond anvil cell, Dias says, opening it up to practical applications. A technique called strain engineering, for example, could mimic the required pressure. In such a process, researchers grow a material on a surface that constrains growth, putting a strain on the material that replicates the effects of externally applied squeezing.
Still, the research faces significant skepticism, in part because of the firestorm over the team’s earlier publication that claimed the discovery of superconductivity in a compound of carbon, sulfur and hydrogen at 15° C (SN: 10/14/20). Editors at Nature retracted that paper, over the objection of Dias and his coauthors, citing irregularities in the researchers’ data handling that undermined the editors’ confidence in the claims (SN: 10/3/22).
Several experts have expressed a lack of confidence in the new results presented by Dias’ group, based on that history. Not only was the previous result retracted, but other researchers were unable to reproduce it, says Eremets, including his own group at the Max Planck Institute. “The main test of validity — reproducibility — was failed, and from my point of view that’s the most important thing.”
The stakes are high. “If it’s true, it’s a great discovery,” says physicist Eugene Gregoryanz of the University of Edinburgh. But he views the researchers with suspicion. “Whether it’s true or not, I guess time will show.”
Others are more positive. “It’s an excellent study,” says materials chemist Russell Hemley of the University of Illinois Chicago. “The data as presented, in terms of evidence for superconductivity, is very strong.” Hemley was not involved with the study but has collaborated with Dias in the past, including on a follow-up to the retracted superconductor paper. Submitted February 16 at arXiv.org, that paper, which has not yet passed peer-review, reports that the previously claimed superconductor does function near room temperature.
The new superconductor is a hydrogen-rich type known as a hydride. Scientists predict that pure hydrogen should be a room-temperature superconductor, but only at extremely high pressures that make it difficult to produce. To lower the pressure, scientists have added in other elements, making hydride superconductors.
In 2015, Eremets and colleagues produced a compound of sulfur and hydrogen that was superconducting up to −70° C, a record high temperature at the time (SN: 12/15/15). A few years later, a compound of lanthanum and hydrogen was found to superconduct under still chilly conditions, but even closer to room temperature (SN: 9/10/18). Both materials require pressures too high for practical use.
It’s difficult to understand how the new superconductor fits in with other hydrides. Theoretical calculations of how similar hydrides behave wouldn’t suggest that such a material would be superconducting at the reported temperatures and pressures, says theoretical physicist Lilia Boeri of the Sapienza University of Rome. “For me, it looks very strange,” Boeri says. “It’s something completely unexpected…. If it’s true, it’s very different from the other hydrides.”